

Obesity has been recognised as one of the leading health concerns in our society (World Health Organization [WHO], 2018). Evidence suggests that good health is at risk for those individuals who live with BMI>30 kg/m² (Herring et al, 2010; Russell et al, 2010; Furness et al, 2011; Heslehurst et al, 2013; Foster et al, 2014). However, obesity rates continue to rise, and obesity remains prevalent both nationally and globally (WHO, 2015; Scottish Public Health Observatory, 2018), multi-factorial reasons have been cited for this such as diets high in obesogenic foods and sedentary lifestyles (Vandevijvere et al, 2018).
Living with a raised BMI>30 kg/m² while pregnant carries risks for both women and their babies that can lead to poor pregnancy outcomes for both and risk the ongoing health of the off spring (Catalano et al, 2009; Denison et al, 2009; Denison and Chiswick 2011; Drake and Reynolds, 2014; Stirrat and Reynolds, 2014; MBRRACE-UK 2014; 2018; Keely, 2015). Evidence suggests that the continued prevalence of obesity in pregnant women will impact upon future generations, who will, in turn, experience the incumbent risks of obesity and sub-optimal health. It is likely, therefore, that the ongoing cycle of obesity will continue to impact on the costs of future healthcare provision.
Midwives, as the first professional point of contact for many women, have a key role to play in providing appropriate evidenced-based advice regarding lifestyle choices of which diet, physical activity and weight management are a few (Dunkley-Bent, 2004). Furthermore, providing women with dietary and physical activity advice has been found to improve maternal health and pregnancy outcomes (Jewell et al, 2014; McGiveron et al, 2014; Ronnberg et al, 2014; Haby et al, 2015). Raising the topic of and maintaining dialogue with women about obesity has been found to be challenging, with professionals being fearful of offending women (Furness et al, 2011; Macleod et al, 2013; Wilkinson et al, 2013; Foster and Hirst, 2014). Research was undertaken to gain deeper understanding of community midwifery practice and how appropriate information is provided to obese women in South East Scotland.
Antenatal care in South East Scotland
Community midwives who took part in this study are based in various health centres and GP surgeries, and ensure that every woman in every geographical area has access to midwifery services. During the antenatal course, the community midwife is responsible for providing holistic care to women, ensuring that appropriate referrals are made to specialists when risks are identified or deviations from normal occur, ensuring appropriate care is provided (NHS Quality Improvement Scotland, 2009; NHS, 2017).
Aim of research study
The aim of the research was to gain deeper understanding about how community midwives practice with respect to raising the topic of obesity and to explore how they maintained dialogue with women about this. Community midwives are well placed to discuss complex health issues with women and their families throughout pregnancy and in the postnatal period of which living with a raised BMI is one. Prior to commencing the research, a narrative literature review was undertaken, the findings of which informed the study design.
Literature review
The literature search aimed to identify literature that reported on professional practice with respect to caring for and advising obese pregnant women. Figure 1 outlines the search strategy that was utilised during this review. The literature was reviewed using questions adapted from Greenhalgh (1998) for quantitative papers, and Walsh and Downe (2006) for qualitative papers. A total of three dominant themes were found (Table 4); midwives perceived that they lacked proficiency in advice giving, midwives were fearful of damaging the midwife/woman relationship, midwives had received insufficient education (about obesity as a topic).
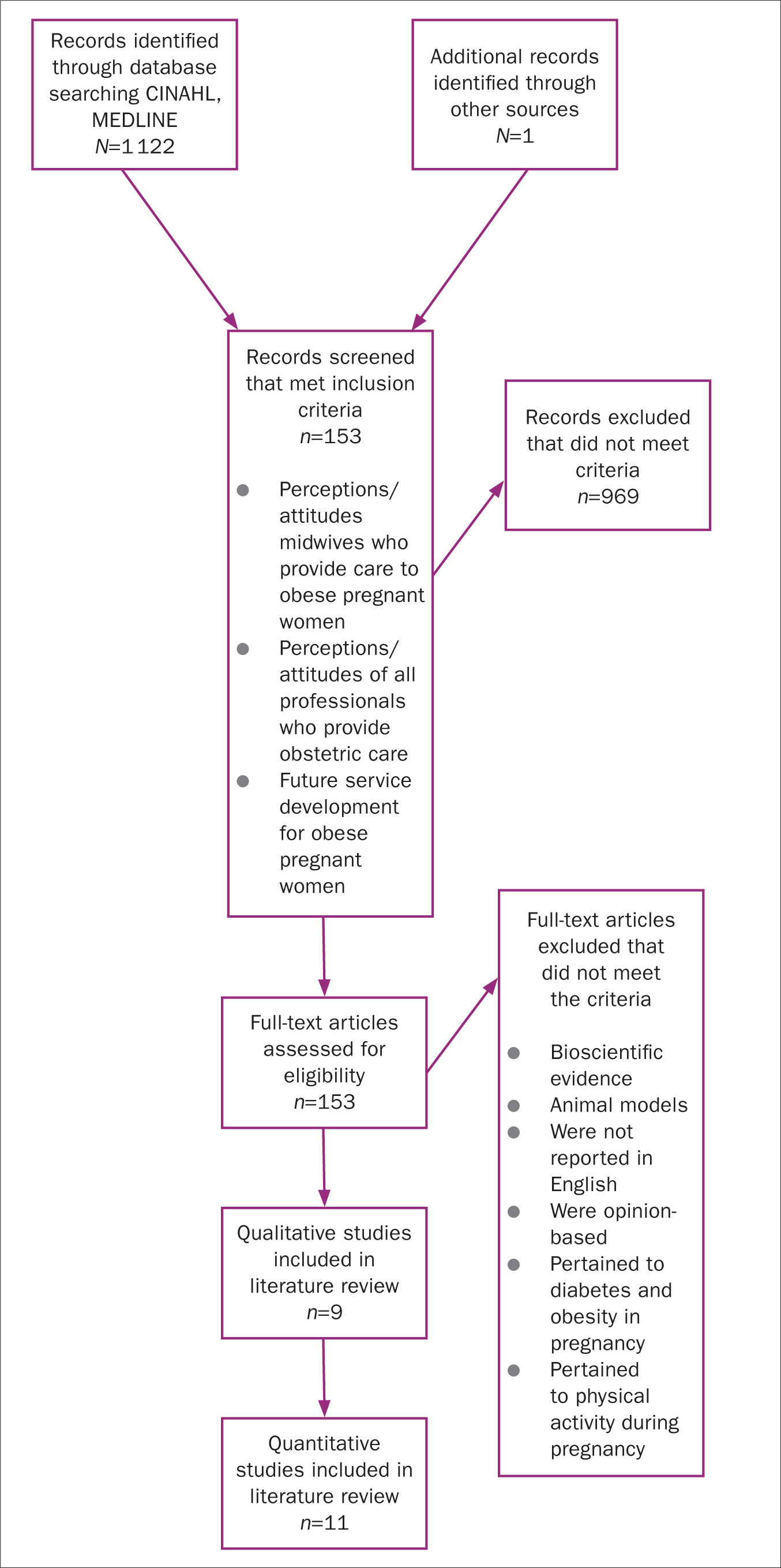 Figure 1 PRISMA chart summarising literature search strategy
Figure 1 PRISMA chart summarising literature search strategy
Table 1. Summary of maternal risks when a woman is obese during pregnancy
| Risks to obese pregnant women |
|---|
|
Table 2. Risks to the fetus when a mother is obese
| Risks to the pregnancy where a mother is obese |
|---|
|
Table 3. Risks to the newborn where the mother is obese
| Risks to the newborn where the mother is obese |
|---|
|
Table 4. Summary of findings from the literature review
| Number of papers | Years of publication | Key findings | |
|---|---|---|---|
| Qualitative research (professional practice) | 9 | 2010–2017 |
|
| Quantitative research (professional practice) | 11 | 2010−2015 |
Ethical approval
Ethics approval for this study was gained from the Higher Education Institution (HEI) and Research and Development department of the NHS Health Board (R&D 2017/0316) where the investigation was to be undertaken, NHS ethical approval for this study was not required because no service users were asked to participate.
Recruitment
Initially, face-to-face meetings were held with community midwifery teams, information sheets were distributed to individuals for them to consider and a follow-up call was made to them after a 24-hour period asking if they would like to participate. Extra information sheets were left in each office to allow those who had been off duty on the day of the visit, ensuring that the research was effectively advertised. Two midwives made contacted with the researcher as a result of this strategy and participated in the study. In total, 13 practicing community midwives consented to take part. A summary of participant characteristics can be seen in Table 1.
Data collection
Data were collected from January to May 2018. Following written and ongoing consent, in-depth interviews were chosen as the data collection method and midwives were also provided with a practice diary asking them to reflect upon up to five episodes where they had provided care to women who had a BMI≥30 kg/m². Interviews lasted between 20–65 minutes. The interview schedule was informed by the initial narrative literature review focusing upon professional practice and advice giving in the context of caring for obese pregnant women (Herring et al, 2010; Stotland et al, 2010; Smith et al, 2012; Willcox et al, 2012; Heslehurst et al, 2013; Knight-Agarwal et al, 2014). Interviews were transcribed verbatim and data were analysed thematically; data from the practice diaries were also analysed thematically.
Philosophical underpinning
This study drew on the pr inciples of social constructionism, a philosophy rooted in the social sciences (Franklin, 1995; Burr, 2015; Gergen, 2015) that is concerned with the ‘language’ and ‘traditions’ of particular groups (Gergen, 2015). Gergen (2015) refers to the ‘game of words’ and suggests that individual groups may all have constructed particular ‘languages’ and ‘behaviours’, and that the meanings of particular words, phrases and actions may differ in different contexts.
Community midwives in South East Scotland are currently ‘based’ in community settings such as GP surgeries and work both independently and remotely from their hospital-based colleagues. They are often the first point of contact for pregnant women (NHS Quality Improvement Scotland, 2009) in Scotland. It is possible that the consequences of this contextual situation where midwives meet women (often for the first time) and aim to concurrently raise sensitive topics and build supportive relationships may be influential in ‘constructing’ language, practices and behaviours that are unique to community practice and influence how professional conversations develop.
Data analysis
An iterative, seven-stage, step-wise approach was developed (Table 6) (Miles and Huberman, 1994; Gibbs, 2007; Harding, 2019) and data were interrogated, observing for language, traditions and behaviours of midwives as they interacted within their contextual situation (Gergen, 2015). Interrogation of the data continued at each stage of analysis, with observance for unique linguistical and behavioural nuances continuing. Three overarching themes were developed that encompassed key elements of community practice: the contextual situation of practice, constructing relationships with women and the midwife as a public health agent. The data were further analysed and interpreted and sub-themes developed. A summary of these themes and sub-themes can be seen in Table 7.
Table 5. Summary of participant characteristics
| Participant name* | Length of community experience | Area of practice** |
|---|---|---|
| Anna | 15 years | Urban – mixed deprived and affluent population |
| Beth | 17 years | Semi-rural – mainly deprived population |
| Catriona | 4.5 years | Urban – mixed deprived and affluent area |
| Denise | 1 year | Urban – mixed deprived and affluent area |
| Elaine | 14 years | Urban – deprived area |
| Frances | 25 years | Rural – deprived area |
| Gaynor | 17 years | Urban – deprived area |
| Heather | 4 years | Urban – affluent area |
| Issy | 6 years | Urban – mixed deprived and affluent population |
| Julia | 5 years | Urban – mixed deprived and affluent population |
| Kat | 20 years | Urban – mixed deprived and affluent population |
| Linda | 1 year | Urban – deprived area |
| Mandy | 3 years | Rural – mixed deprived and affluent population |
Description of area of practice from Scottish Index of Multiple Deprivation (2018)
Table 6. Step-wise approach to data analysis
| Stage of analysis | Progress of analysis (descriptive to analytical) |
|---|---|
| 1. Transcripts made | To allow familiarisation with the data |
| 2. Transcripts read and re-read | To allow for an overview of the findings/themes that were emerging |
| 3. Colour coded in the hard copies and preliminary themes identified | Four dominant broad themes identified |
| Original highlighted excerpts assigned a category or node | |
| 4. Uploading of transcripts in to NVivo 10 computer programme | Nodes expanded and the data were interrogated again with a focus on observing for differences and similarities in views and practices |
| 5. Line-by-line analysis observation of the transcripts | Observing for linguistical nuances that allowed for deeper understanding and meaning to be elicited from the data |
| 6. Preliminary themes identified | Four themes identified pertaining to practice, organisational expectations and societal change |
| 7. Return to hard copies to re-engage with the data. Line-by-line analysis repeated observing for language, context and tradition | Three over-arching themes identified; constructing relationships with women*, the situational context of practice and the midwife as a public health agent |
Table 7. Summary of key findings
| Main theme | Situational context of practice | Constructing relationships and partnerships with women | Midwives as public health agents |
|---|---|---|---|
| Sub-themes 1 | Blending the paradigms of midwifery and obstetric practice | Developing an effective partnership with women | Mode of delivery (public health messages and messengers) |
| Sub-themes 2 | ‘The protocols say’—risk to exercising professional judgement | Information exchange between midwife and woman | ‘I think they want us to give everything priority’ |
| Sub-themes 3 | I just don't know! (enough about the topic) | ‘[Feeling] so time constrained.’ Time constraints leading to being unable to hear the woman's full story |
Findings: constructing relationships with women
Midwives appeared to prioritise the development of respectful and trusting relationships with women and their families during the pregnancy and understand that they had a professional duty to provide evidence-based advice:
‘…You have to get their trust, you have to get their respect as the midwife for that first appointment and you can engage them and they feel and they think you're of value to them as the midwife and that you're educating them and can give them good advice then you're on their side and they'll come back but if you alienate them at that first appointment and start lecturing them and you know…’ (Frances)
However, the subject of weight and weight management appeared to be viewed as a sensitive one that some midwives veered away from for fear of causing offence to women in their care:
‘…I don't actually have a problem with it [discussing having a raised BMI] because I really feel it's a benefit to them that eh … I think it's a benefit to them in that we … because they are at huge risk, that we can hopefully reduce this risk and that we'll pick up problems sooner rather than later…’ (Anna)
‘…at that initial meeting, you are trying to build up that relationship and the last thing you want to do is annoy…’ (Catriona)
The above two quotes demonstrate that despite understanding the potential consequences of being obese, tensions arise for professionals that appear to inhibit meaningful discussion.
Midwives turned to relevant clinical protocols as a ‘way in’ to the conversation and viewed these documents as ‘giving permission’ for them to raise sensitive topics of which living with a BMI≥30 kg/m² is one:
‘…Yes, yes, because it's not me having a pop at you. It's me being told this is what I have to do by clinical guidance from the hospital. Then makes them go [name]'s not having a pop at me and saying I'm fat…’ (Elaine)
Using protocols in this way, however, inhibits the development of autonomous practice and suggests that some midwives may be missing opportunities to explore lifestyle choices such as diet, weight maintenance and physical activity, all of which have been shown to improve outcomes for pregnancy, labour and birth (Jewell et al, 2014; McGiveron et al, 2014; Haby et al, 2015). This calls into question their adherence to the code (Nursing and Midwifery Council [NMC], 2018) and their understanding of how to practice autonomously, an element of which is to provide current evidence-based advice to women without first requiring permission to do so.
Despite the existence of clinical protocols, some midwives did appear to develop communication strategies of their own volition, attempting to raise conversations with women about living with obesity:
‘…I just think that's just years and I think realising what works and what doesn't and also the feedback from my women because I have been here for 13 years, a lot of them say that they like the ‘spade-like’ approach that I have…’ (Elaine)
However, when probed, this midwife did acknowledge that her communication style was based on her own assessment of her skills and not on evidence-based models. This calls in to questions whether midwives measure their self-assessment against professional standards and may suggest a lack of self-awareness with respect to their professional communication styles.
Information exchange between midwife and woman
When probed more closely, participants acknowledged that they had learnt ‘communication’ informally and ‘on the job’ as a student and during many years of practice rather than as a result of receiving formal education:
‘…I think as a student you've got such a fantastic position, you're in such a fantastic position because you get to work with different midwives and see how they do things and I was forever, “Oh, I like the way she said that”, “Oh, I like the way she did that”, you know. So you pick up a lot of positive ways of saying things through watching other people and then I think when you qualify you just have to learn what, what your style is but it takes time to do that you know…’ (Linda)
Although there was awareness that individuals used this ‘on-the-job’ approach to develop their communication skills, there appeared to be a lack of insight about various communications styles that are available (Silverman et al, 2013). It is possible that being exposed to educational opportunities that facilitate exploration of these styles may support practice.
‘The protocols say’ the risk to professional judgement
Institutional questionnaires used to record information in the maternity notes appeared to not only provide permission for midwives to raise the topic of obesity, but also to devolve the responsibility for doing so to the institution:
‘…So I say “the computer's just worked out your BMI, were you aware of your BMI, do you know what BMI is?” and just, you know, explore it with them. And they just go, “Well I know I'm a wee bit heavier” or sometimes if it's a second-time mum they'll go, “Well I'm definitely a wee bit heavier than I was in my first pregnancy” … ’ (Frances)
In addition, there were several instances where midwives appeared to utilise these questionnaire as a ‘tick-box’ list, rather than personalising and structuring the appointments ensuring the inclusion of woman-specific topics:
‘…Basically, I wait to the point in the notes where I'm almost given licence to talk about it because Trak [computer programme] has told me to talk about it. And the same goes for any other kind of awkward questions, like you know, the questions about domestic violence, questions about previous drug use or depression or whatever. I ask the question when it actually occurs in the notes…’ (Kat)
This use of questionnaires appears to perpetuate the lack of autonomous practice and facilitates midwives to ‘hide’ behind the questions, suggesting a ‘self-protection’ strategy, although it was not clear what they were protecting themselves from.
Discussion
The importance of the midwife-woman relationship (Foster and Hirst, 2014; Jomeen, 2017; McParlin et al, 2017) is advocated in the professional driver documents as being a positive force in a woman's life (Pathways for Maternity Care, 2009; NHS, 2017; Chief Nursing Officers of England, Northern Ireland, Scotland and Wales, 2020). Participants valued the women-midwife relationship, appearing to prioritise it over delivering evidence-based advice that may optimise the health of mother and baby. These findings mirror other international findings (Heslehurst et al, 2013; Knight-Agarwal et al, 2014; Pan et al, 2015; McParlin et al, 2017). This apparent lack of professional awareness calls into question their compliance with the NMC (2018) code of conduct and their understanding of ‘practise effectively’ concerning their responsibility to deliver evidence-based information.
Participants appeared to pride themselves on being ‘good’ communicators; however, they were unable to articulate how they arrived at this conclusion, calling into question their professional knowledge about the communication of sensitive issues. They appeared to judge for themselves, what was ‘good’ or ‘sub-optimal’ practice prior to developing or constructing their own practice rather than underpinning it with evidence. This suggests that their professional communication skills may not be as effective as they believe. Silverman et al (2013) caution that ‘experience alone can be a poor teacher’ and state that communication education should be as robust as that of any other skill. Provision of targeted education with respect to communication may therefore, strengthen midwifery practice.
Midwives viewed the clinical protocols as providing ‘permission’ to raise ‘sensitive’ topics of which obesity is one. This appeared to allow them to ‘distance’ themselves from the somewhat prescriptive obesity protocol used in the health board (Denison et al, 2016) and the investigations that are advised for obese pregnant women, explaining that these were compulsory requirements rather than being optional. This risks midwifery practice being viewed from a medical perspective. Phrases such as, ‘I have to [instigate various additional investigations] reflect this more medicalised approach, suggesting that women are being failed by midwives who do not always seek informed consent which is a central tenet of healthcare (Chan et al, 2017). This again calls into question their professionalism and adherence to the code (NMC, 2018).
The institutional questionnaires that are utilised to record information during antenatal appointments appear to provide a ‘checklist’ type approach to the antenatal interview. Midwives appear to find this helpful, however, this means that all women are asked the same questions irrespective of their individual needs or wishes. This risks conflating the ‘woman-centred’ appointment to a list of routinised questions that may devalue professional autonomy and lead to ineffective individualised decisions being made (Frain, 2018).
Providing educational opportunities for midwives at both undergraduate and postgraduate levels that facilitate exploration around communication and consultation skills may strengthen and support practice. Recipients of such education may, as a result, develop confidence in raising sensitive issues while concurrently developing effective partnerships with women.
Limitations
This was an exploratory study with 13 practicing community midwife participants. While offering insight into how midwives practice with respect to providing care to obese pregnant women in one geographical location, it is unclear if these findings can be generalised to other areas of practice or geographical areas. All data were collected by one researcher. The views of women were not captured during this study but this was a conscious decision because the research aimed to explore influencing factors for midwifery practice during antenatal appointments. Comparisons between length of experience and practice style was not investigated, doing so may have elicited further insights into practice. While midwives appeared anxious about offending women, none of them raised concerns about having complaints raised against them. Further enquiry about this issue may also have yielded deeper insights.
Conclusion
The observational way in which midwives reported that they learn communication skills may be a weakness in professional practice. Midwives reported that they had not received any formal education around communication although this was not verified with Higher Education Institutions (HEIs). Midwives are failing women by omitting appropriate evidence-based information during appointments for some women. This in turn could risk the good health of mother and baby.
Designing curricula, ensuring that targeted educational components, with respect to communication and consultation skills are included may strengthen midwifery practice and empower midwives to raise and discuss the topic of obesity. However, more work is required to ascertain if this educational need is UK-wide. In addition, the provision of postgraduate educational opportunities by HEIs that will facilitate midwives to develop their communication and consultations skills may be beneficial for those already in practice. Midwives may not be aware that they are contravening the code (NMC, 2018) by not raising and maintaining dialogue about obesity with pregnant women.
Key Points
- Rates of obese pregnant women presenting for maternity care continue to rise
- How midwives raise and maintain dialogue with women about health risks is poorly understood
- Evidence suggests that modifying diet, increasing physical activity and maintaining weight in pregnancy can improve maternity outcomes
- Research was undertaken to gain deeper understanding about how community midwives approach this element of care
- Findings suggest that providing educational opportunities at both undergraduate and postgraduate levels with respect to communication and consultation may strengthen practice and empower midwives to engage in conversations about perceived sensitive topics
CPD reflective questions
- Consider your understanding of the differences between communication and consultation. Are you clear on the definition of either/both?
- What consultation models, if any, are you aware of that could be used to underpin and influence your practice to facilitate effective discussions surrounding obesity in pregnancy?
- How much consideration have you given to the code (NMC, 2018) and how you may be contravening it by avoiding discussion around this topic?
- Considering your earlier answer, how will you adjust your practice for future consultations with obese pregnant women?