

In 2019, the World Health Organization published a strategy that outlined the benefits of simulated learning in nursing and midwifery education (Martins et al, 2019). It focused primarily on the importance of learning goals, scenario design, pre-brief (which can include becoming familiar with the clinical space and equipment), simulation and post-brief learning conversation as key aspects of simulated learning. These principles of educational design are also well integrated into comprehensive standards of simulated practice in healthcare (Purva and Nicklin, 2018; Society for Simulation in Europe, 2019). Likewise, systematic reviews and meta-analyses continue to show the impact of simulated learning on healthcare students' knowledge, confidence, clinical ability, empathy, team working and interdisciplinary learning (Marion-Martins and Pinho, 2020; Mulyadi et al, 2020; Chua et al, 2021; Lei et al, 2022; Silva et al, 2022; Yun et al, 2023; Tonapa et al, 2023). In response to this evidence, although simulated learning does not count towards practice hours in pre-registration midwifery programmes, it has nonetheless been integrated into curriculum designs and therefore requires effective curriculum implementation.
Complementary to the curriculum design process, and ahead of any curriculum evaluation, Hughes (2022) described curriculum implementation as the process by which educationalists creatively consider and plan how the components of the curriculum are going to be administered; so that curriculum design as a ‘mental exercise becomes a reality’. While there are multiple aspects to curriculum implementation such as the people, facilities, resources and administration, design thinking and the resulting implementation (referred to as design actions) remains central features (Wrigley and Straker, 2017). When it comes to simulated learning as a component of a midwifery curriculum, it is important that the design actions, and the learning theories that underpin them, are documented. Yet Bajpai et al (2019) highlighted how existing literature lacks sufficient evidence that outlines the relationship between overall curriculum design and the learning theories intended to lead to the desired curriculum outcomes (evaluation). The aim of this article is to begin to address this gap by sharing the theoretical design of the three main design actions related to implementing simulated learning into a BSc in Midwifery programme. The article will present the reason why motivational theories are a theoretical underpinning for the implementation of simulated learning and describe the three key design actions and their underpinning motivational theories.
Motivational theory for implementing simulated learning in midwifery
There is good evidence for simulated learning in respect to students' learning gain, satisfaction and overall self-confidence (Marion-Martins and Pinho, 2020; Mulyadi et al, 2020; Chua et al, 2021; Lei et al, 2022; Silva et al, 2022; Yun et al, 2023; Tonapa et al, 2023). Although there are multiple factors that must converge to positively influence students' motivation to learn (Keller, 2008), the role of student satisfaction and self-confidence are important determinants of the degree of intrinsic motivation students will experience. Intrinsic motivation in particular, is known to be a strong driver of a student's creativity, openness to learning and overall positivity towards the learning experience (Sansone and Harackiewicz, 2000). In contrast to extrinsic drivers and rewards, intrinsic motivation is also associated with the mechanism of psychological safety (Ali et al, 2022).
According to Nakayama et al (2018), healthcare students can lack psychological safety during simulation. Psychological stress that is simulation-induced is associated with students' anticipation of a critical event, the thought of being observed and the risk of publicly displaying a lack of skill and/or knowledge to perform (Bhoja et al, 2020). To counter the risk of simulation-related stress, educators are challenged to create a ‘psychologically safe’ learning experience, where students will feel at ease to master the challenge being set (Daniels et al, 2021).
Psychological safety is when participants feel comfortable and do not experience embarrassment or worries about speaking up, sharing their thoughts or asking for help, according to Roh et al (2021). In addition, Turner et al (2023) found when researching psychological safety that students felt safe when they had a relationship with their sim facilitators, who knew their abilities and so refrained from judging their performance unfairly. However, considering what is known about intrinsic motivation and its association with psychological safety (Ali et al, 2022), there is a premise for a more systematic application of motivational theories at a curriculum implementation level.
There are multiple motivational design models that can enable and guide educators in the design of motivating learning experiences, of which the most commonly applied is Keller's (2010) ARCS-V model. Although motivational design models are underpinned by theories, they are designed mainly to guide educators in solving particular learning challenges, such as motivating students to learn about perinatal mental health interdisciplinary care planning (Stockdale et al, 2023). When considering how learning theories influence the implementation of a curriculum component, Bajpai et al (2019) recommended more explicit identification of which learning theories are being applied and how. In a curriculum, knowing this information not only guides the creation of design actions, but also provides a theoretical foundation for evaluating what works, when and how at the curriculum evaluation stage.
Designing implementation of a curriculum with high-fidelity simulation
Hughes et al (2022) descr ibed cur r iculum implementation as a step that begins once curriculum development is completed. In reality, pre-planning for implementation often commences prior to completion of the curriculum development process. An added advantage of starting the design thinking process early is that the gap between the written and implemented curriculum can be minimised (Karakus, 2021).
In order to incorporate simulation in the midwifery programme, a simulation expert midwifery group was established, whose first challenge was to evaluate which design actions would support implementation of high-fidelity simulation in the undergraduate midwifery programme. Led by the simulation lead for midwifery in the university, the group consisted of one senior practising midwife from each trust, two practice education midwives, academics interested in simulation, teaching assistants (who were registered midwives) and student representatives. Practising midwives were nominated by the NHS trusts while the students submitted a successful expression of interest. Unlike the wider curriculum-development group, whose remit would end with the approval of the curriculum, the simulation expert group continues to guide and drive implementation of the simulation component of the midwifery curriculum. To ensure that the proposed innovations were theoretically driven, an academic with knowledge of motivation to learn facilitated the initial discussions.
Three main design actions were identified by the group. Two design actions originated early in the design thinking process. The skills passport was proposed and included in the curriculum document, but was only built and implemented as part of the curriculum implementation plan following approval. The third design action was added to the plan in year two of curriculum implementation. However, in each instance, the simulation design actions were underpinned by the theories of motivation to learn.
Design action 1: students' confidence and scaffolded learning
According to Keller (2010), there are multiple psychological theories and concepts that explain students' confidence and how it can be influenced, such as their perceptions of control and predictability of the learning experience captured, their beliefs related to expected success and how they interpret their perceived successes and failures. Theorists Linnenbrink and Pintrich (2000) highlighted that students who approach a learning challenge with the goal of mastering it, referred to as mastery-orientation, are much more likely to experience confidence in the form of self-efficacy. This in turn creates motivation to apply ongoing effort and persistence until the goal is achieved. Underpinned by a belief that ability grows over time, students who are mainly mastery-orientated are therefore those who are also committed to their own development and improvement, even if their progress is slow (Keller, 2010).
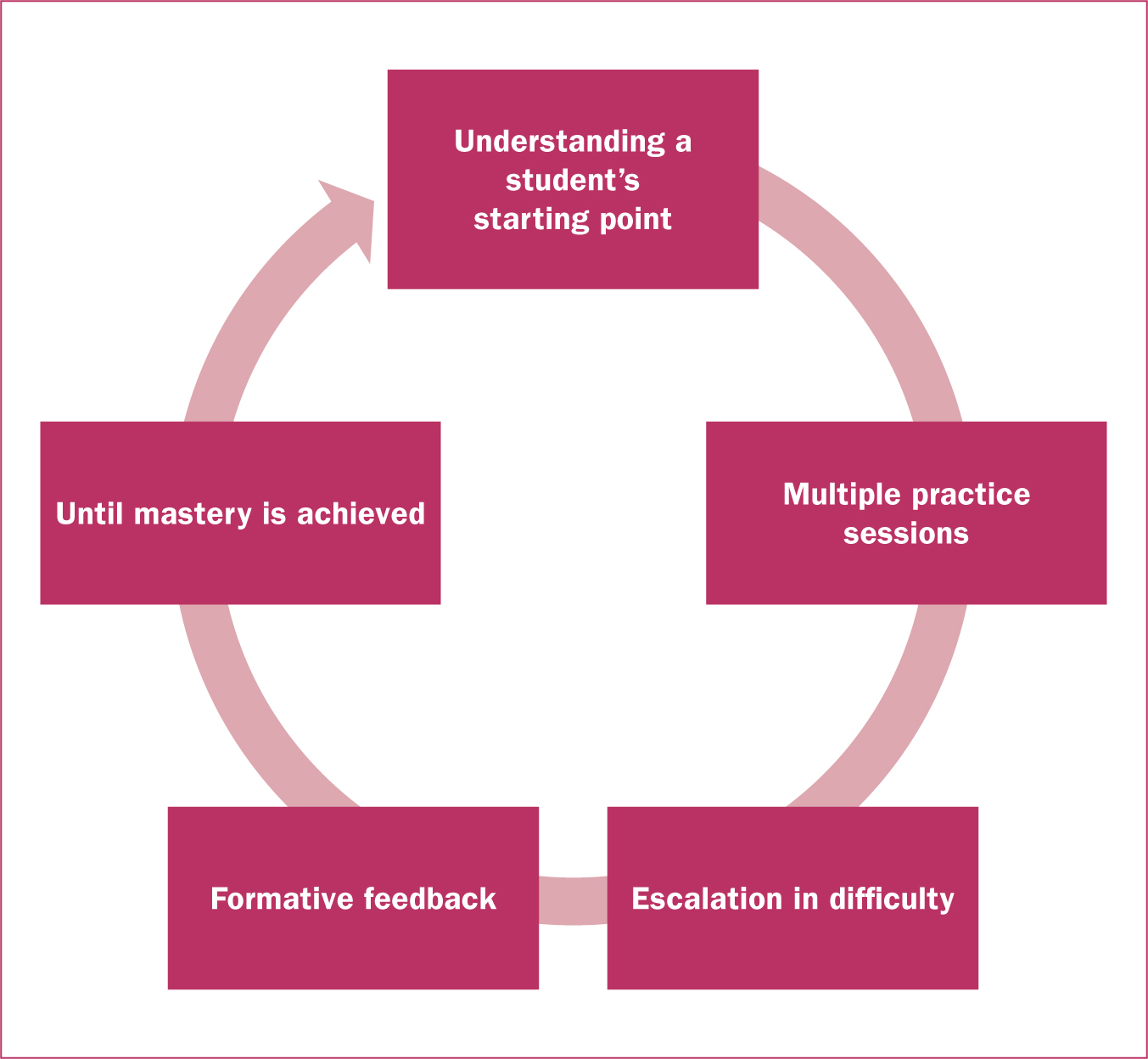
Mastery-orientated learning is well accepted in relation to simulated learning, on the basis that it increases the psychological safety of learners and therefore, their overall learning (Dunn et al, 2017; McGaghie et al, 2020; Reeder et al, 2021). Recommending the implementation of mastery-orientation, Felix and Schertzer (2022) drew educators' attention to the importance of scaffolding (Figure 1). Based on Vygotsky's (1978) theory of scaffolding, the authors recommended that this cycle includes a gradual fading of support until the students become independently successful (the goal is mastered).
When it comes to integrating simulation into midwifery education, the Nursing and Midwifery Council (2018) standards framework for nursing and midwifery education (part 1, updated in 2023) requires that students' simulated learning experience is an empowering and enabling one that is scaffolded in terms of contributing, participating and demonstrating skilled practice. Aiming to provide this, the team began with scaffolding the experience of simulated learning within the three already approved scaffolded skill modules in the curriculum. As outlined in Table 1, the year one skills module was designed to focus on students' participation in skilled care (starting point); year two focused on students' contribution (ongoing mastery); and year 3 focused on their demonstration that mastery was achieved (performance).
Table 1. Outline of the scaffolded modules at a curriculum level
| Module title | Simulation-related learning outcomes (goals) | Assessment design |
|---|---|---|
| Learning to participate in skilled midwifery practice | Describe and apply communication and teamworking principles in providing safe and effective maternity care | Short written case management report and presentation that challenges students to connect their learning with the provision of care |
| Contributing to skilled midwifery practice | Use self-evaluation and team reflection to optimise communication in providing safe and effective maternity careUse evidence-based decision making in co-production with women and other professionals | Digitalised case study and presentation to peers/clinicians |
| Demonstrating proficiency in skilled midwifery practice | Demonstrate the provision of universal and additional care and critically examine interdisciplinary team working Use self-awareness in providing person-centred, safe maternity services | Reflective instant report of a team response to an obstetric emergency (including review of the demonstrated human factors) and a summative team simulation |
Achieving scaffolded learning is a necessary foundation for simulated learning; however, two key scaffolding considerations also directed implementation at a module level. First, setting the level of the simulated challenges in each year, so that students' confidence and mastery remained optimal in the lead up to their summative simulation (performance). Second, introducing human factors education early and at a level that matched the sim challenges that students would be set. For example, as simulations became more complex, this demanded higher performance from the student teams in terms of their situational awareness, leadership and followership.
How considerations were reflected at a module level
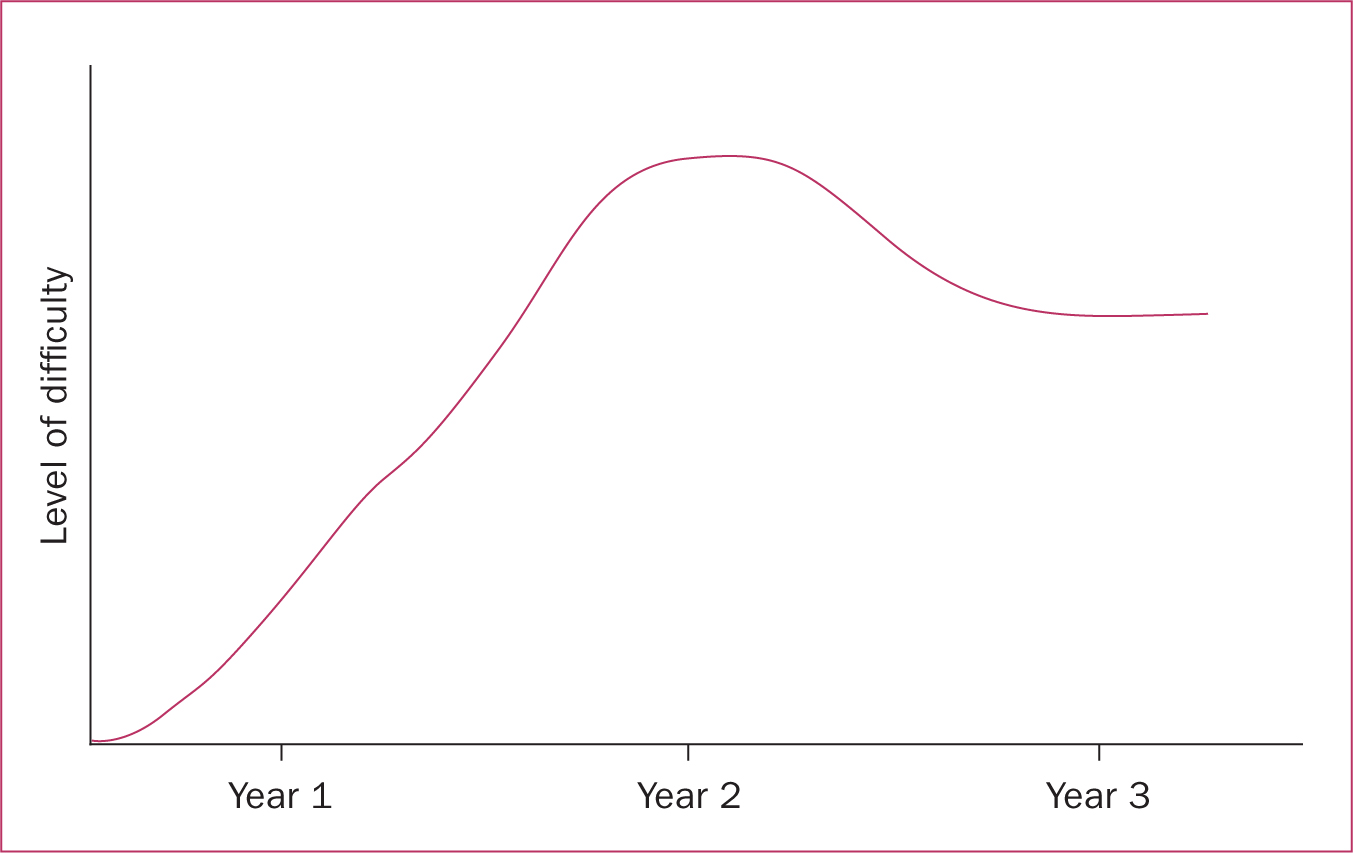
In setting the level of challenge, taking the literature at face value led to the temptation to simply increase the difficulty of the simulations year on year, up until the point where students demonstrated mastery through a summative sim in year 3 (Figure 2). However, it was recognised that this design overlooked the accepted principles of the Yerkes Dodson Law (Keller, 2010). The law demonstrates that there is a curvilinear relationship between learners' ongoing motivation to learn (mastery) and their demonstration of mastered performances. Students' motivation and related performance only increases to a point; then students will begin to lose their motivation to learn, negatively affecting their performance.

If a simulation were perceived to be too easy for students (high-confidence state), then their motivation to learn would be negatively affected, as they would not perceive a sense of challenge nor the need to learn. Conversely, if the simulation were over-challenging, then in this context, the students' low-confidence state would likely to lead to disengagement, as they perceive a sense of helplessness in being able to learn. To ensure that students' simulated learning experiences remained motivating and therefore mastery-orientated, it was important that the design team considered the level of challenge set and implemented in each year. Guided by the scaffolding outlined at a curriculum level, a non-linear approach to the level of difficulty was implemented (Figure 3) where the level of simulation fidelity steadily increased during year one, reached a peak at the end of year 2 and then levelled off in year 3.
When matching the simulation with human factors education, it was important to understand that for a healthcare team to provide safe and effective care, they need to have knowledge of human factors and how it influences their team's performances. Although simulation was designed to be introduced in year one, there was a realisation that human factors education would have to be scaffolded to match the level of fidelity. Table 2 describes the degree of fidelity and the associated human factors education provided.
Table 2. Year of study and description of scaffolded simulated challenge
| Year of study | Level of challenge and rationale |
|---|---|
| Year 1: learning to participate in skilled midwifery practice | Simulation challenge levels are restricted to scenario-based universal care. Before immersing themselves in the simulation, students undergo a thorough pre-briefing that empowers them to collaboratively plan how to deliver care in a team-orientated experience. As this is the students' starting point, there is recognition that students need to be exposed to simulation to learn how to immerse into it, suspending their disbelief (Richardson et al, 2022). To enable immersion, they need exposure to clinical practice where they observe midwives in action. Therefore, the level of challenge is set to steadily increase over the year, culminating with an introduction to scenario-based simulation of mild postpartum haemorrhage as the closing simulation. Human factors knowledge is restricted to communication in terms of situation-background-assessment-recommendation for escalation and simple task completion for teamworking |
| Year 2: contributing to skilled midwifery practice | Simulation challenge levels increase significantly, on the assumption that students have had:
|
| Year 3: demonstrating proficiency in skilled midwifery practice | In year 3, the challenge level is reduced in relation to the degree of fidelity experienced; students are no longer exposed to coming on duty in a maternity unit. Instead, in preparation for their summative simulation, mastery-orientated learning gradually begins to focus on the role of human factors in establishing high performing teams. The focus on performance orientation combined with their experience in mastery is in preparation for their summative simulation. Unlike years 1 and 2, year 3 uses a structured and systematic approach to learning about human factors. Applying the model by Rosenorn-Lanng (2014), students are challenged to demonstrate their knowledge of the systems, human interactions, environment, equipment and personal factors as determinants of high performing healthcare teams. Placed in teams of four at the beginning of the year, the students experience scenario-based simulations that challenge them to implement their knowledge of human factors. This is both through real-time simulations in the InterSim Centre and technology-supported simulations (video-based) |
Design action 2: students' self-regulation (volition) and the skills passport
Panadero et al (2017) published a series of helpful meta-analyses that outlined the relationship between students' self-assessment of their own work, self-regulatory behaviours that support their ongoing learning and the degree of self-efficacy or confidence-based motivation, that they experience. Discussing self-assessment, the authors emphasised that students who only follow what an educator ‘prescribes’, without learning to self-assess and adjust their learning approach according to their own progress, are not productive and effective learners. However, when students do self-assess, they are more likely to generate self-regulatory beliefs and actions, such as being more goal and task focused, reflective and effort-orientated in relation to their perceived successes and failures (Zimmerman, 2000). The more self-regulatory behaviours students adopt, the greater the impact on their self-efficacy, in that they become conscious of their own improving competencies. In turn, the motivational effect of this perceived competency is increased effort, persistence and overall improved performance. In 2008, Keller (2008) proposed an integrated theory that not only captured this series of events between students' self-regulation and their willingness, effort and persistence to learn, but also how this motivational process could be influenced by the educators' design of the learning experience. With this theoretical knowledge at hand, it became apparent that students' growth through simulation would also motivationally benefit from having some form of self-assessment related to their skills development.
Through discussions in the simulation expert working group, it was recognised that students require an appropriate level of combined skills to experience optimal learning via any scenario-based, high-fidelity simulation. It became apparent that a skill-based, self-assessment intervention was required. Different than the electronic midwifery record of achievement (eMORA, the official practice-based assessment tool), it was anticipated that this innovation would be fully controlled by the individual student, providing them with specific developmental goals related to each skill (including top tips for implementing the specific skill) and an area for their own notes and reflections about their progress. For easy access, it was decided that the skills passport should be accessible to students via the eMORA platform.
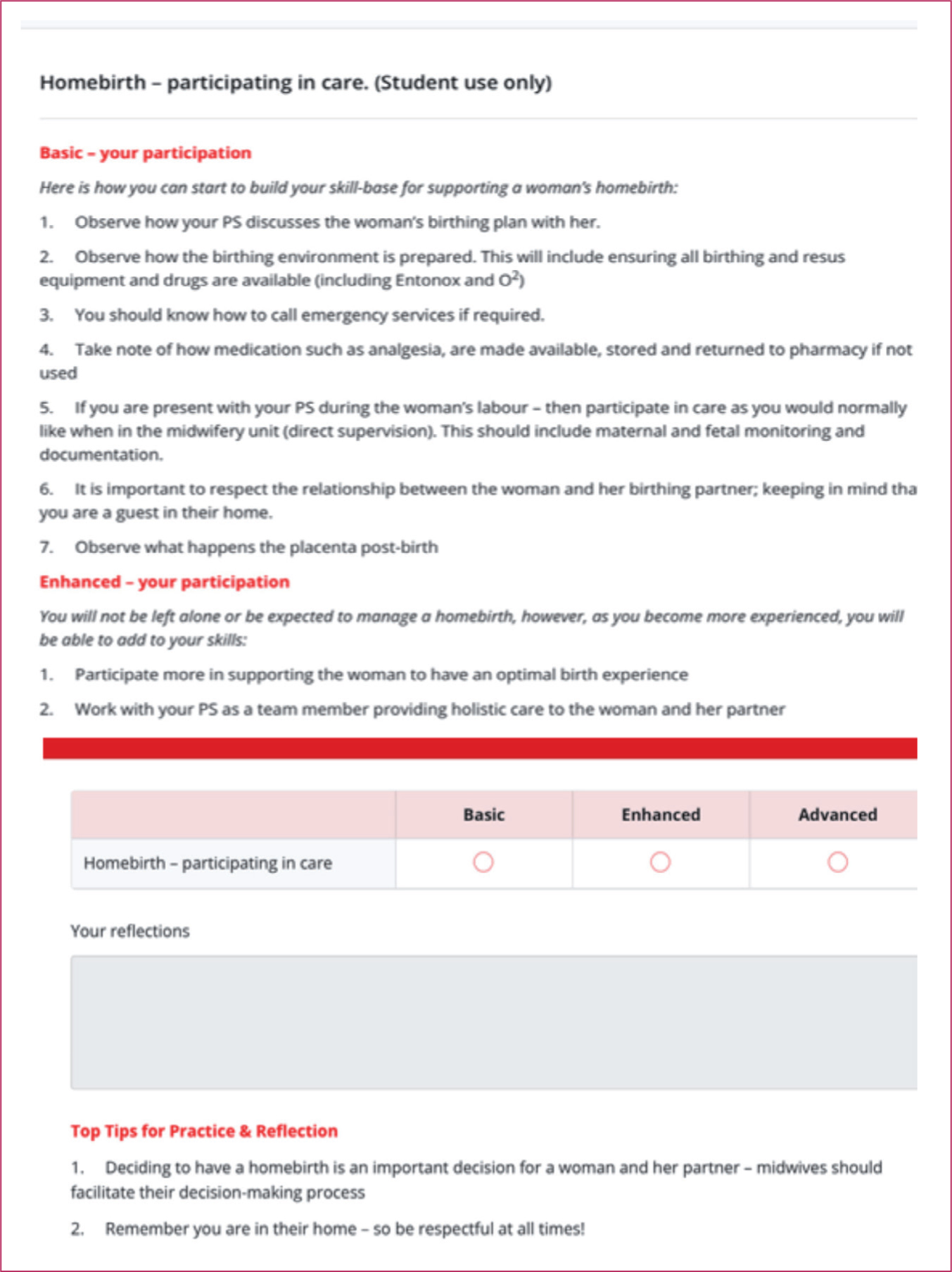
Led by the midwifery simulation group, co-production of the content in Skills Passport was extended to other expert midwives from across all trusts; for example, a midwifery expert in perinatal mental health designed the information on recognising and responding to a woman presenting with perinatal anxiety. Taking an all-trust approach ensured that expectations were realistic and standardised for what skills students should aim to achieve at different stages of their education. This process approach also enabled a clear mapping of all midwifery skills, including those that were less obvious; for example communicating with a woman via an interpreter or contributing to a woman's care in the absence of a fetal heart. Currently, there are over 100 skills alphabetically listed in the student-led skills passport. As the example in Figure 4 demonstrates, the skills are not catalogued according to student year, but by the level of students' ongoing skill development (simulation only, basic, enhanced and advanced). This scaffolded structure was designed to enable flexibility in relation to students' individualised skill development, as not all students develop all skills at the same pace as a result of variation in exposure. This also meant that some skills could be restricted to a certain level; for example, the skill of breaking unexpected news was restricted to simulation only. An example from the skills passport, learning to develop skills in relation to a homebirth, is shown in Figure 4. The example illustrates the different levels of goal orientation, the opportunity for students to self-monitor each time they are exposed to the skill and self-assess in relation to reflection on their progress. It is anticipated that skill development will continue beyond that expected of undergraduate students, as students transition to becoming newly qualified midwives.
Action 3: Schwartz rounds and students' approach-orientated motivation
Scholars have long recognised that the curriculum, though written and approved, requires continuous, timely and relevant implementation (Lieff, 2009). As students began to experience the newly approved curriculum, they engaged in simulation with other disciplines, where they learned about Schwartz rounds. Originating in the USA, Schwartz rounds were first introduced into the NHS in 2009 (Taylor et al, 2018). Their purpose is to provide healthcare professionals with a psychologically safe place where they can discuss the emotional and social aspects of their roles, so preventing compassion fatigue, burnout and consequently, less impactful care (Maben et al, 2021; Ng et al, 2023). The benefits of Schwartz rounds include reduced stress, strengthened multidisciplinary teams (including student teams), increased empathy for those being cared for and compassion for self and other team members (Barker et al, 2016; Robert et al, 2017; Maben et al, 2021; Ng et al, 2023). In consultation with students, the simulation expert working group introduced Schwartz rounds as a third design action related to psychological safety (Smith et al, 2020).
As already noted, there is evidence of an association between psychological safety and intrinsic motivation that implies when people feel intrinsically satisfied, they will also feel more psychologically safe. Schwartz rounds indirectly add to what is known about this association by focusing on a theoretical understanding of emotion, stress and social psychology; when healthcare professionals experience shared understanding and so feel emotionally supported, they are less likely to withdraw from the challenges that they are experiencing (George, 2016; Maben et al, 2021). Motivational theorists such as Elliot et al (2013) have long agreed that emotion can be better understood from a motivational position, in particular, emotion can be seen in whether a person is motivated to approach or to avoid a challenge. In other words, emotion is not in itself a phenomenological experience, but part of a more complex and often hidden motivational process that will either energise and direct an individual to approach a challenge, or de-energise and direct them to avoid the challenge.
Through Schwartz rounds, healthcare professionals have an opportunity to experience trust and containment, enabling their storytelling, self-disclosure, contextualisation, reflection and ultimately their motivation to persist, demonstrated through improved teamwork, tolerance, empathy, openness and compassion (Maben et al, 2021). As the benefits of Schwartz rounds develop slowly over time, the simulation expert working group agreed that midwifery students, alongside medical and nursing students, should be engaging in Schwartz rounds as part of their simulated learning experience. To enable this, two midwifery academics completed Schwartz facilitation training prior to introducing year three midwifery students to the rounds. A short evaluation with this cohort of students is currently underway in order to inform further scaffolding for introduction to year one and two midwifery students.
Conclusions
Implementing simulation in an undergraduate midwifery curriculum requires careful planning. A theory-guided approach that results in well-defined design actions are recommended, as this works to close the gap between a written and implemented curriculum.
In terms of learning theories, the association between motivation and psychological safety can be an important element of designing how simulated learning will be implemented in a curriculum. However, to ensure pragmatic implementation of theory, a simulation expert working group, consisting of educationalists, practitioners and students, is recommended. Through collaborative design thinking, the most relevant design actions can be identified. For the midwifery curriculum described, this included scaffolding for confidence building, a skills passport for self-regulated learning and Schwartz rounds for approach-orientated motivation. As the first cycle of curriculum implementation approaches, the theoretical basis for the outlined design actions provides a foundation for evaluating what works, when and how for midwifery students experiencing simulated learning across a midwifery curriculum.
Key points
- Motivational theory provides a useful guide when integrating simulated learning across the curriculum.
- Establishing an expert working group is important when implementing simulation, which should discuss the appropriate application of motivational learning theories to develop the key design actions.
- Three design approaches are most useful: increasing student confidence through scaffolding learning, using a skills passport to increase students' self-regulation, and encouraging approach-orientated learning through interdisciplinary Schwartz Rounds.
CPD reflective questions
- Reflecting on the role of motivation to learn, how have you scaffolded the level of simulated challenge for your students?
- Giving students control over how they develop as a skilled practitioner is important. How do you encourage students to be self-regulated?
- On reflection, do your students tend to demonstrate their desire to approach or avoid simulation, and what does that tell you as an educator?